Back to resources
Turmeric vs. Curcumin: Moving Beyond the "Blanket Remedy"
Deep dive about turmeric and curcumin, including the core distinctions between the whole root and the extract, the inflammatory pathway illustrations, and the clinical caution around formulation and dosing.
Introduction
In my clinical practice, I frequently encounter patients who have proactively added turmeric or curcumin to their daily regimen. It is encouraging to see such widespread interest in natural anti-inflammatories, but there is often a gap between simply taking a supplement and using these botanical tools with clinical precision.
While the terms are often used interchangeably in casual conversation, understanding the distinction between the whole rhizome and its isolated constituents is essential when the goal is a specific therapeutic effect rather than a vague sense of support.
The key clinical question is not whether turmeric is "good." It is whether the form, concentration, and delivery method actually match the physiology you are trying to influence.
The Whole and the Part: Definitions
To use these tools effectively, we first need to distinguish the source from the extract.
- Turmeric ( Curcuma longa ): the whole root, or rhizome. It contains over 200 molecular compounds, including volatile oils, polysaccharides, and fiber. Turmeric powder usually contains only 2 to 5 percent curcuminoids by weight.
- Curcumin: the primary curcuminoid found in turmeric. It is the best-studied "active ingredient" and is responsible for much of the plant's yellow pigment and many of its systemic pharmacologic effects.
That distinction matters because the whole plant behaves differently than a standardized extract. The whole root functions more like a broad botanical and culinary support, while a concentrated curcuminoid extract behaves more like a targeted intervention.
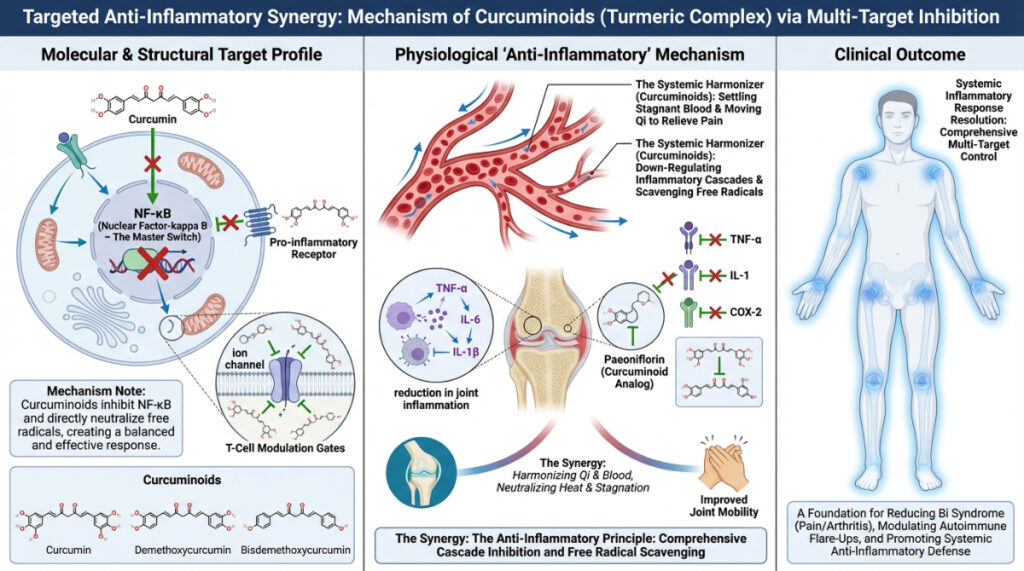
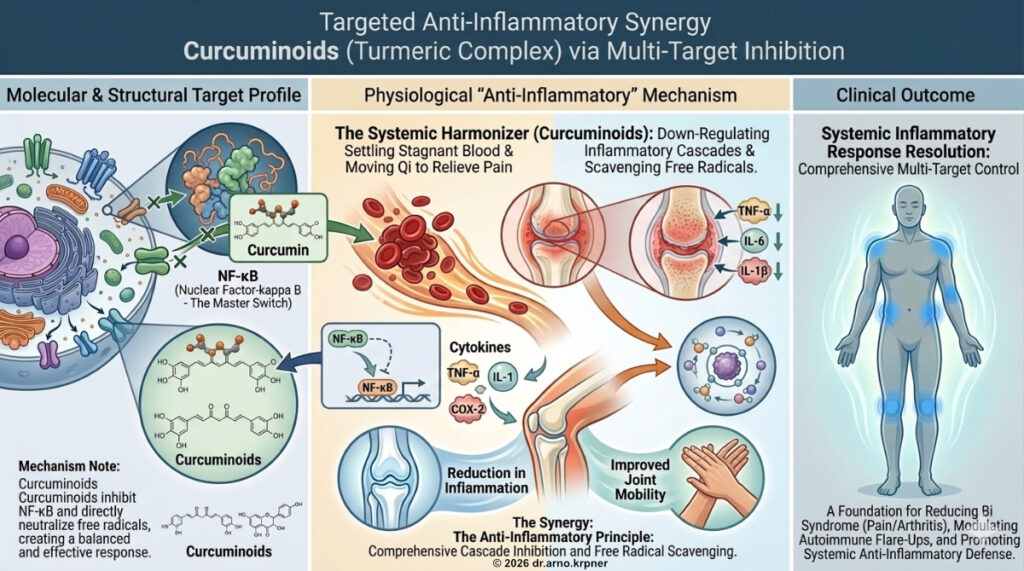
The Biochemical Pathway: Addressing Inflammation
The primary mechanism involves inhibition of Nuclear Factor-kappa B, or NF-kappa B. This protein complex acts like a master switch for inflammation. When activated, it enters the cell nucleus and turns on genes that produce inflammatory cytokines.
From a modern physiologic perspective, curcumin acts as a multi-target molecule. Unlike NSAIDs, which mainly inhibit COX-2, curcumin modulates inflammatory signaling further upstream.
By suppressing NF-kappa B, curcumin can reduce the expression of:
- Cyclooxygenase-2 (COX-2) and 5-Lipooxygenase (5-LOX)
- Tumor Necrosis Factor-alpha (TNF-alpha)
- Interleukins such as IL-1, IL-6, and IL-8
Integrative Perspectives: TCM and Functional Medicine
Functional Medicine
In Functional Medicine, curcumin is often used as a tool for metabolic detoxification and oxidative stress management.
- Phase II Detoxification: curcumin can induce Nrf2, a pathway that increases the production of endogenous antioxidants such as glutathione.
- Intestinal Permeability: it is often used to support the gut barrier and modulate the gut microbiota, both of which influence systemic immune health.
Traditional Chinese Medicine (TCM)
In the Materia Medica, we distinguish between Jiang Huang , the turmeric rhizome, and Yu Jin , the tuber. Turmeric is characterized as acrid, bitter, and warm.
- Blood Invigoration: it is used to break up Blood Stasis, especially in the shoulders and joints.
- Qi Movement: it helps move stagnant Qi and alleviate pain.
- The Warmth Factor: because it is warm, it tends to fit Cold patterns of pain better than Heat or Yin-deficient patterns.
Functional Medicine and TCM use different language here, but both are really asking the same thing: where is the terrain blocked, inflamed, overloaded, or unable to resolve properly?
The Importance of Extract Concentration and Bioavailability
One of the most common mistakes in self-supplementation is ignoring pharmacokinetics. Raw turmeric powder has notoriously low bioavailability. Much of the curcumin is rapidly metabolized and excreted before meaningful systemic levels are reached.
To move from a blanket remedy to a true clinical intervention, formulation matters:
- Concentration: therapeutic extracts are often standardized to 95 percent curcuminoids.
- Adjuvants: piperine from black pepper can markedly increase absorption by slowing metabolic clearance.
- Liposomal or phytosome delivery: binding curcumin to lipids can improve systemic availability, especially for more targeted applications like neuroinflammation or cardiovascular support.
This is one reason a patient may feel that "turmeric didn't work" when the real issue was not the botanical itself, but the mismatch between the product, the dose, and the physiologic target.
Clinical Safety: When "Natural" Requires Caution
As powerful as these extracts are, they are not inert. Because curcumin can act as a mild blood harmonizer or anticoagulant, I advise patients to consult their care team if they are taking:
- Blood thinners such as warfarin, clopidogrel, or DOACs, because of a potential increase in bleeding risk.
- Diabetes medication, because curcumin may further lower blood glucose.
- Upcoming surgery, since I generally advise discontinuing use about 14 days before a procedure.
Even though curcumin may support digestion, its cholagogue effect means it should be used carefully, or sometimes avoided, in people with active gallstones or certain biliary issues.
Conclusion
Turmeric is a remarkable whole food and culinary medicine. Curcuminoids are a more concentrated class of extracts. But when we are targeting chronic inflammatory pathways or specific Blood Stasis patterns, dosage, concentration, and delivery method determine whether the intervention actually works.
If you are using these tools, they should ideally be matched to your specific biology and clinical picture rather than used as a generic supplement trend.