Chronic kidney disease is never just about creatinine. It changes
inflammation, vascular resilience, mineral balance, mitochondrial
function, and often the entire feeling of how the body is coping.
Chronic kidney disease affects hundreds of millions of people
worldwide and still remains underdiagnosed until later stages.
That delay matters because the kidneys do far more than filter
waste. They help regulate fluid balance, blood pressure, mineral
handling, acid-base status, hormone signaling, and the larger
chemistry of recovery.
As kidney function declines, the body does not simply become
"less efficient." It enters a more burdened physiological state
where inflammation, metabolic waste, vascular stiffness, anemia,
fatigue, and structural strain begin to reinforce each other.
The practical frame:
CKD should be managed with nephrology-level seriousness, but it
is also useful to understand it as a whole-body systems problem
rather than an isolated organ story.
What chronic kidney disease actually is
Chronic kidney disease is the gradual loss of kidney function
over time. In conventional medicine this is often tracked
through estimated glomerular filtration rate, creatinine,
albuminuria, blood pressure, and the broader pattern of
diabetes, hypertension, vascular disease, or structural kidney
injury.
Those markers matter, but they do not always capture the lived
experience of the patient. People often feel fatigue, reduced
exercise tolerance, itching, fluid instability, cognitive
dulling, appetite shifts, sleep disruption, or a general loss of
resilience before they fully understand what the kidneys are no
longer handling well.
CKD changes much more than filtration. Energy, fluid handling,
mineral balance, and cardiovascular strain all become part of
the picture.
Why CKD becomes a whole-body problem
When kidney function falls, metabolic waste products accumulate
more easily. Fluid and electrolyte handling become less stable.
The pressure on the cardiovascular system rises. Over time, that
can drive deeper fatigue, higher inflammatory tone, endothelial
dysfunction, bone-mineral disruption, and a greater sense that
the body is working harder for less return.
Energy:
patients often experience profound fatigue and reduced
exercise recovery.
Transport:
blood vessels and blood pressure regulation become more
strained.
Structure:
bone-mineral handling shifts, increasing the risk of
brittleness and vascular calcification.
Communication:
hormonal and metabolic signaling become less coordinated.
This is why kidney disease so often overlaps with cardiovascular
risk, metabolic instability, and a feeling of accelerated aging.
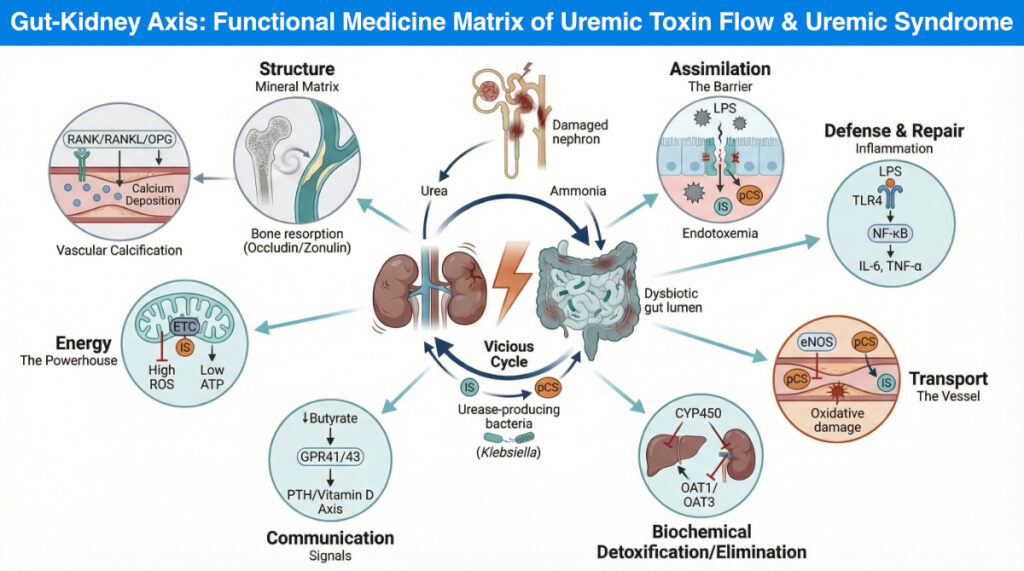
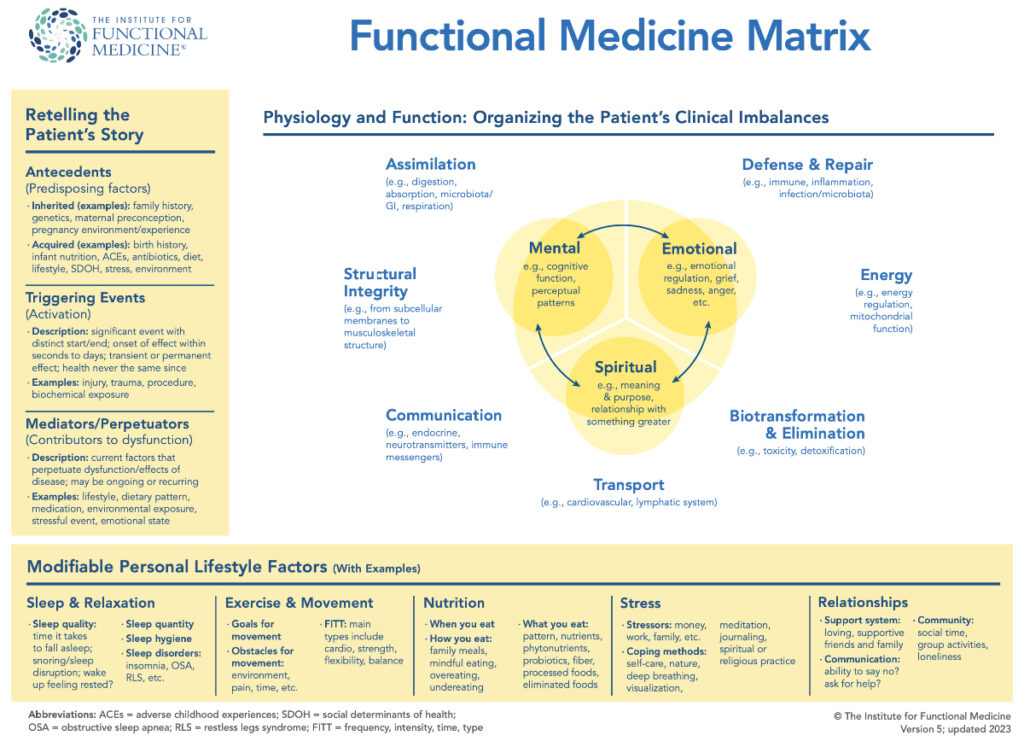
The functional medicine matrix and the gut-kidney axis
A systems-based lens can be useful here because it helps explain
why so many symptoms appear outside the kidneys themselves. In
functional medicine, CKD can be understood through a matrix of
assimilation, defense and repair, transport, biotransformation,
communication, energy, and structure.
The matrix view helps organize how CKD spills into digestion,
inflammation, vascular function, energy production, and
structural health.
One of the most interesting and clinically relevant pieces is
the gut-kidney axis. As kidney clearance declines, the
intestinal environment changes. Dysbiosis becomes more common,
the gut barrier can become more vulnerable, and inflammatory
compounds generated in the gut may circulate more freely. That
combination can increase systemic inflammation and amplify the
burden on an already stressed system.
Why this matters:
digestive terrain, fiber tolerance, microbial balance, and
inflammatory load often matter more in CKD than patients are
initially told.
Where the clinical burden tends to show up
When CKD advances, the body often reveals the strain through
several recurring channels:
Inflammation and immune stress:
ongoing exposure to uremic toxins and gut-derived inflammatory
signaling can keep the immune system activated.
Vascular risk:
endothelial dysfunction, arterial stiffness, and hypertension
become harder to separate from the kidney disease itself.
Mitochondrial strain:
reduced cellular energy availability can contribute to the
deep exhaustion many patients describe.
Mineral misplacement:
calcium and phosphorus handling can shift in ways that weaken
bone and harden blood vessels.
Medication complexity:
detoxification and medication handling can become less
forgiving as renal function declines.
A good clinical plan respects all of these at once. Otherwise,
the person gets treated as a lab trend instead of as a living
system under pressure.
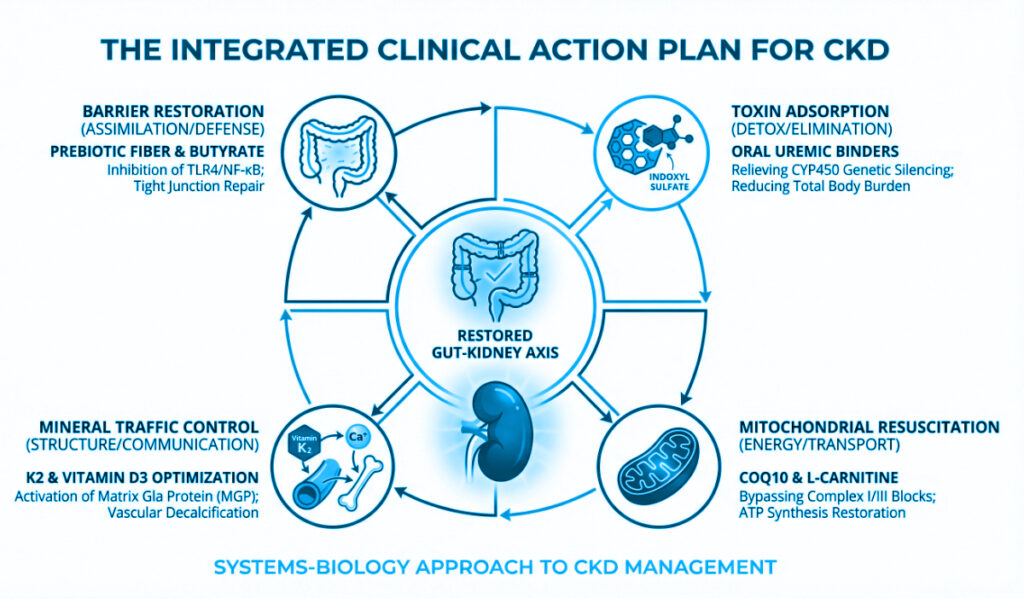
What supportive integrative care can realistically focus on
Integrative care is not a replacement for nephrology, blood
pressure management, diabetes care, or medication safety. It
can, however, help support the terrain around the disease. That
usually means reducing inflammatory burden, supporting digestive
resilience, improving nutrient adequacy, protecting
mitochondrial function, and making everyday physiology less
chaotic.
Gut support:
fiber strategy, bowel regularity, and microbiome support may
help lower systemic inflammatory burden when used
appropriately.
Metabolic steadiness:
glucose control and blood pressure control remain central
because they strongly influence progression.
Mitochondrial support:
carefully selected nutrients may help with fatigue and
cellular stress in the right patient.
Mineral and vitamin guidance:
vitamin D, K2, magnesium, and phosphorus-related questions all
require individualized interpretation in CKD.
The goal is not generic supplementation. It is a more coherent
plan around inflammation, recovery, nutrient handling, and
daily physiological stability.
What needs real caution
CKD is an area where well-intended wellness advice can become
risky quickly. Some herbs, minerals, "detox" protocols,
high-protein plans, dehydration-based fasting, and unsupervised
supplement stacks can worsen the situation rather than improve
it. That is especially true once kidney function is clearly
reduced or medications are already in play.
The safest mindset is collaborative: nephrology for disease
monitoring and medical management, and a broader integrative
frame to reduce total body burden without creating new harm.
Important:
any supportive plan in CKD should be checked for medication
interactions, stage-specific safety, electrolyte consequences,
and renal dosing concerns.
The larger point
CKD can feel like a diagnosis of decline, but it is also a
condition where clarity matters. When we understand the links
between kidney function, gut health, inflammation, vascular
strain, energy, and structure, we gain a better map for what can
still be supported.
That map does not promise reversal in every case. It does create
a more intelligent way to think about fatigue, progression risk,
symptom burden, and the practical steps that can make the
terrain less hostile over time.