Methylation is one of the most discussed and misunderstood
concepts in functional medicine. The real clinical question is not
whether someone has an isolated “methylation issue,” but how B12
status, metabolic stress, gut function, inflammation, and cellular
resilience fit together.
Patients now routinely arrive convinced they have “methylation
problems,” often because direct-to-consumer genetics or internet
discussions have turned MTHFR, methyl donors, and detoxification
into a kind of biochemical mythology. The reality is more
interesting and more clinically useful.
From a systems perspective, methylation is not a single switch
that gets turned on with supplements. It is a dynamic network
tied to nutrient sufficiency, mitochondrial energy production,
inflammation, gastrointestinal function, hormonal signaling,
oxidative stress, nervous-system regulation, and environmental
load.
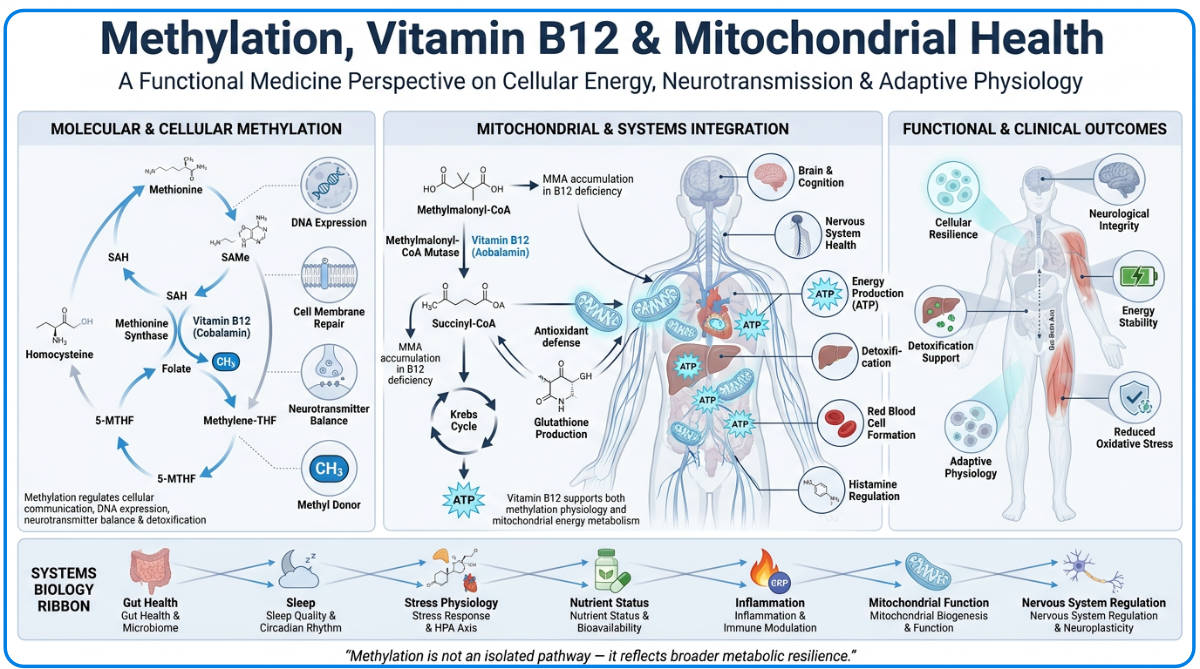
The practical frame:
methylation is best understood as a reflection of broader
metabolic resilience, not as a standalone diagnosis.
What methylation actually does
Methylation refers to the transfer of a methyl group from one
molecule to another. That simple act influences a remarkable
range of physiology, including DNA expression, neurotransmitter
metabolism, phospholipid integrity, hormone metabolism,
histamine clearance, creatine synthesis, myelin maintenance, and
mitochondrial energy production.
The physiology is tightly linked to three major pathways: the
methionine cycle, the folate cycle, and the transsulfuration
pathway. Together they connect methyl donors, homocysteine
recycling, glutathione production, oxidative stress handling,
and cellular adaptation under load.
Methionine cycle:
regulates SAMe generation and homocysteine handling.
Folate cycle:
provides methyl groups for homocysteine recycling.
Transsulfuration:
supports glutathione synthesis and antioxidant defense.
Why vitamin B12 matters far beyond “energy”
Vitamin B12 plays a central role in both methylation physiology
and mitochondrial metabolism. It is essential for neurological
integrity, red blood cell formation, fatty acid metabolism, DNA
synthesis, and ATP-relevant mitochondrial reactions.
Functionally, B12 is less about whether someone consumes enough
in theory and more about whether they can absorb, transport,
activate, and use it. That is why functional deficiency can
occur even when intake appears adequate.
Methylcobalamin:
linked more directly to methylation and homocysteine
recycling.
Adenosylcobalamin:
linked more directly to mitochondrial metabolism and energy
production.
Absorption depends on:
stomach acid, intrinsic factor, pancreatic function, ileal
integrity, and healthy enterohepatic recycling.
Why serum B12 alone can mislead
Conventional evaluation often assumes that serum B12 reflects
true sufficiency. In practice, serum B12 is only a circulating
marker. It does not reliably tell you whether B12 is getting
into cells, being converted properly, or being used effectively
in the tissues that matter.
A patient can have normal serum B12, or even elevated serum B12,
while still showing signs of functional deficiency.
Inflammation, altered binding proteins, liver dysfunction,
transport issues, oxidative stress, and impaired cellular uptake
can all distort the picture.
This is why functional interpretation often broadens the lens to
include methylmalonic acid, homocysteine, CBC patterns such as
MCV, folate, iron studies, renal function, and above all the
symptom pattern.
MMA and homocysteine: useful, but only in context
Methylmalonic acid is one of the most useful markers for
functional B12 status because intracellular B12 is required to
convert methylmalonyl-CoA into succinyl-CoA. When that reaction
slows, MMA rises. In many cases it becomes abnormal before overt
hematologic findings appear.
Homocysteine is also useful, but it is frequently
overinterpreted. It behaves more like a metabolic stress signal
than a standalone diagnosis. It can rise with B12, folate, B6,
or riboflavin insufficiency, but also with thyroid dysfunction,
kidney strain, inflammation, oxidative stress, genetics, and
broader metabolic burden.
Elevated MMA may suggest:
functional intracellular B12 deficiency, early tissue
deficiency, or mitochondrial metabolic strain.
Elevated homocysteine may suggest:
impaired methylation capacity, but also oxidative burden or
broader physiology under stress.
Both still require context:
symptoms, CBC patterns, renal function, inflammatory tone, and
the larger clinical story.
The MTHFR problem on the internet
MTHFR variants such as C677T and A1298C are common. They are
not, by themselves, proof of severe dysfunction, failed
detoxification, or an automatic need for high-dose methylfolate.
Genes matter, but they express themselves inside a physiological
environment.
In practice, many people who believe they have “methylation
problems” are actually dealing with broader upstream stressors:
gastrointestinal dysfunction, chronic inflammation, sleep loss,
nutrient insufficiency, oxidative stress, environmental load,
alcohol exposure, mitochondrial strain, or nervous-system
dysregulation.
The functional medicine objective is not to “fix genes.” It is
to support the terrain in which those genes are operating.
Common upstream contributors
B12 and methylation dysfunction often emerge as downstream
reflections of digestive, inflammatory, nutritional, or
medication-related pressures. Clinically, the work becomes far
more effective when these are identified early.
Why aggressively “pushing methylation” is often a mistake
One of the most common mistakes in modern functional medicine is
to respond to every methylation discussion with high-dose methyl
donors. Some people benefit. Others become more anxious,
overstimulated, or biochemically destabilized.
Symptoms such as insomnia, irritability, palpitations,
headaches, agitation, or sensory overload do not necessarily
mean methylation support is wrong. More often they suggest the
terrain is not ready for aggressive intervention, the dosing is
excessive, or the deeper physiology has not been stabilized
first.
The goal is not to force pathways biochemically. The goal is to
restore enough metabolic resilience that the pathways can
regulate themselves more effectively.
Foundational supports usually matter more than supplement
enthusiasm: protein sufficiency, mineral status, sleep quality,
blood sugar stability, circadian rhythm, gastrointestinal
integrity, inflammatory burden, and nervous-system regulation.
How I think about this clinically
Methylation is best interpreted as a systems-level reflection of
how the body is allocating resources under stress. When someone
presents with fatigue, neuropathy, brain fog, macrocytosis, mood
changes, or detoxification intolerance, I am less interested in
chasing a single SNP than in asking what the larger metabolic
environment looks like.
That means looking at symptoms, serum B12, MMA, homocysteine,
CBC patterns, renal function, digestive integrity, medication
history, inflammatory load, mitochondrial resilience, and the
patient’s overall capacity to adapt. Only then does
supplementation make sense as part of a larger strategy rather
than as a biochemical shortcut.
A broader biochemistry view helps show why methylation, B12,
mitochondrial function, oxidative stress, and nervous-system
regulation should not be interpreted in isolation.