Back to resources
Omega-3s: why they still matter
The more I gather and evaluate research for clients, the more omega-3s keep showing up. They remain one of the most consistently relevant nutritional inputs across cardiometabolic, inflammatory, and neurocognitive health.
What omega-3s are
Omega-3 fatty acids are polyunsaturated fats that play an important role in human physiology. The three forms with the most clinical relevance are ALA (alpha-linolenic acid), EPA (eicosapentaenoic acid), and DHA (docosahexaenoic acid).
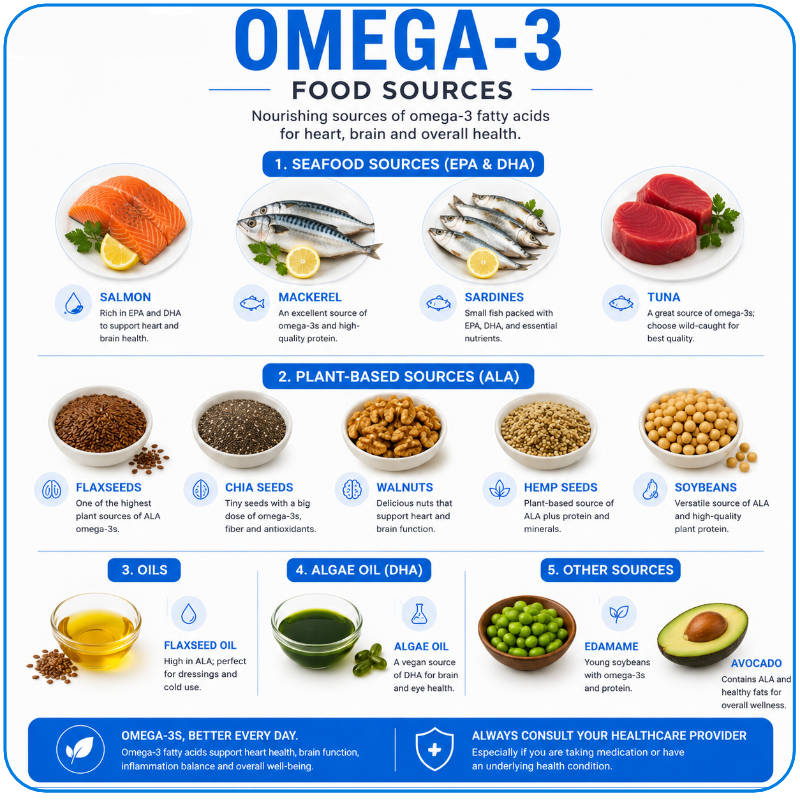
ALA is found mainly in plant foods such as flax, walnuts, and seeds. EPA and DHA are concentrated in marine sources such as fish, fish oil, algae, and the organisms lower in the food chain that fish consume.
Fifty years ago, the early Inuit research helped push omega-3s into the cardiovascular discussion. Since then, the story has widened far beyond heart disease into inflammation, neurocognition, immune regulation, respiratory health, and broader mortality risk.
Omega-3s are not a niche supplement topic. They sit at the intersection of inflammation, membrane biology, vascular function, and long-term resilience.
Why EPA and DHA are clinically different
EPA and DHA share structural similarities, but they are not interchangeable in practice. They participate in pathways involved in blood clotting, inflammation, cell signaling, vascular tone, and heart rhythm stability.
ALA still has value, but its relevance is different. EPA and DHA tend to be the forms that matter most when we are talking about actual tissue levels, omega-3 index targets, and the clinical effects people are often trying to achieve.
What about the omega-6 to omega-3 ratio?
Omega-6 fats are often vilified, but that framing is too simple. The more practical issue for most people is not aggressively cutting every omega-6 source. It is failing to achieve adequate omega-3 status in the first place.
Rather than obsessing over the ratio in the abstract, it is usually more useful to ask whether EPA and DHA exposure is actually high enough to move tissue levels into a healthier range.
How much omega-3 is enough?
Public health advice often settles on two servings of fish per week, which works out to only a modest daily average. That may be enough for general nutrition messaging, but it is often not enough to produce the tissue levels associated with stronger cardiometabolic benefit.
In the original newsletter, I pointed out that a combined daily EPA and DHA intake between roughly 1.75 and 2.5 grams can help many people move toward an omega-3 index around 8 percent, a level often associated with better outcomes.
| Stage of life | Adequate intake noted in the newsletter |
|---|---|
| Birth to 1 year | 500 mg daily |
| 1 to 3 years | 700 mg daily |
| 4 to 8 years | 900 mg daily |
| 9 to 13 years | 1,200 mg for males and 1,000 mg for females daily |
| 14 to 18 years | 1,600 mg for males and 1,100 mg for females daily |
| Adults | 1,600 mg for males and 1,100 mg for females daily |
| Pregnancy / lactation | 1,400 mg daily in pregnancy and 1,300 mg during lactation |
Those numbers are not the same thing as individualized therapeutic dosing, but they are a useful baseline. In practice, I often care more about measured tissue status and the clinical context than about generic supplement labels.
The omega-3 index is the more useful long-term marker
The omega-3 index measures the fatty acid concentrations in red blood cells rather than in plasma alone. That makes it a better reflection of longer-term exposure and tissue incorporation.
In that sense, it behaves more like an A1C does for glucose than like a one-off dietary snapshot. The newsletter highlighted data showing that higher blood concentrations of EPA and DHA were associated with lower all-cause mortality as well as lower cardiovascular and cancer mortality in pooled analyses.
Do omega-3s create bleeding problems?
Omega-3s do have blood-thinning effects, which is why this concern keeps coming up. But the picture is more nuanced than the fear suggests. The newsletter pointed out that the effect on bleeding time is in the range of what people accept routinely with aspirin, and some perioperative data even suggest lower blood loss rather than worse outcomes.
That does not mean dosing no longer matters or that medication context should be ignored. It does mean that the blanket fear around omega-3s and surgery is often overstated.
The more useful clinical question is not “Are omega-3s dangerous?” but “What is the dose, what else is the patient taking, and what is the actual goal?”