Back to resources
Understanding Peyronie's Disease & Treatment Options
Peyronie's disease is a distinct urological condition characterized by the formation of fibrous scar tissue within the tunica albuginea. This article includes the tables and clinical figures.
Introduction: Contextualizing the Disease
Peyronie's disease (PD) is a distinct urological condition characterized by the formation of fibrous scar tissue, known as plaque, within the tunica albuginea of the penis. This plaque, which is fundamentally different from arterial or dental plaque, interferes with the elasticity of the penile tissue, leading to a bent or curved erection, penile pain, and potential shortening.
The disease is classified as a wound-healing disorder, a categorization that aligns it with other fibrotic conditions like keloids and Dupuytren's contracture. While PD is most prevalent in men aged 40 to 70, its exact epidemiology remains limited.
The precise etiology of PD is not fully understood, but it is believed to be the result of a multifaceted process. The most widely accepted theory posits that repetitive micro-trauma or injury to the penis, often occurring during vigorous sexual activity, triggers an aberrant wound-healing response. However, a significant number of patients cannot recall a specific traumatic event.
The impact of PD extends far beyond its physical manifestations. The condition can lead to significant psychological and emotional distress, including stress, anxiety, and depression, with some reports indicating that as many as 77% of men with the disease experience notable psychological effects.

Peyronie's disease is not just a curve. It is a wound-healing disorder with physical, sexual, and psychological consequences.
The Biphasic Clinical Course: Active vs. Stable Disease
A fundamental principle in the management of PD is the distinction between its two clinical phases: the active inflammatory phase and the chronic stable phase. This biphasic nature is the most critical factor in determining the appropriate treatment strategy.
The active phase, which can last for up to 18 months, is characterized by dynamic and changing symptoms, including pain with or without erection, and a gradual worsening of the penile curvature. Following the active phase, the disease transitions into the stable phase, which is clinically defined by the resolution of pain and the stabilization of the penile curvature and plaque size for a minimum of three to six months.
Table 1. Peyronie's disease staging and management
| Clinical Stage | Defining Characteristics | Recommended Management Strategy |
|---|---|---|
| Active/Inflammatory Phase | Dynamic symptoms, pain with or without erection, changing penile curve, duration typically less than 12-18 months. | Observation, pain management such as NSAIDs, intralesional injections, and penile traction therapy. Goal is to prevent disease progression and reduce pain. |
| Chronic/Stable Phase | Pain has resolved, penile curvature and plaque size have been stable for at least 3-6 months. | Intralesional injections such as collagenase, penile traction therapy, or surgical correction. Goal is to correct deformity and restore function. |
Diagnostic Evaluation: Laying the Clinical Foundation
A thorough diagnostic evaluation is essential for effective management of Peyronie's disease. The initial assessment begins with a focused medical and sexual history, which should include the duration of symptoms, the presence and severity of penile pain, the degree and direction of deformity, and any associated erectile dysfunction.
A physical examination of the genitalia is also mandatory to palpate for the presence of a fibrous plaque and to assess for related conditions, such as Dupuytren's contracture or Ledderhose disease of the plantar fascia.

Non-Surgical Treatment Modalities: Management of Active and Chronic Disease
A variety of non-surgical treatments are available for Peyronie's disease, with the most appropriate option depending heavily on the disease stage and patient-specific factors.
Oral Therapies
Historically, numerous oral agents have been used to treat PD, but a shift towards evidence-based practice has led to a re-evaluation of their efficacy. Major clinical guidelines largely do not recommend oral therapies for the significant reduction of penile curvature or plaque size.
Intralesional Injection Therapy
Intralesional injections involve the direct administration of a therapeutic agent into the penile plaque, offering a more targeted approach than systemic oral medications.
Collagenase Clostridium Histolyticum (CCH) - XIAFLEX
Collagenase Clostridium histolyticum (CCH), marketed as XIAFLEX, is the only drug approved by the FDA for the treatment of PD. It is indicated for men with a palpable plaque and a penile curvature between 30 and 90 degrees. Clinical trials have demonstrated modest yet significant efficacy, with a mean curvature reduction of 23 degrees and an average improvement of 38 percent.

Verapamil and Interferon-a2b
Other intralesional agents, such as verapamil and interferon-a2b, are considered off-label treatments for PD. Their use persists in practice, but the evidence remains more limited and mixed than for collagenase.

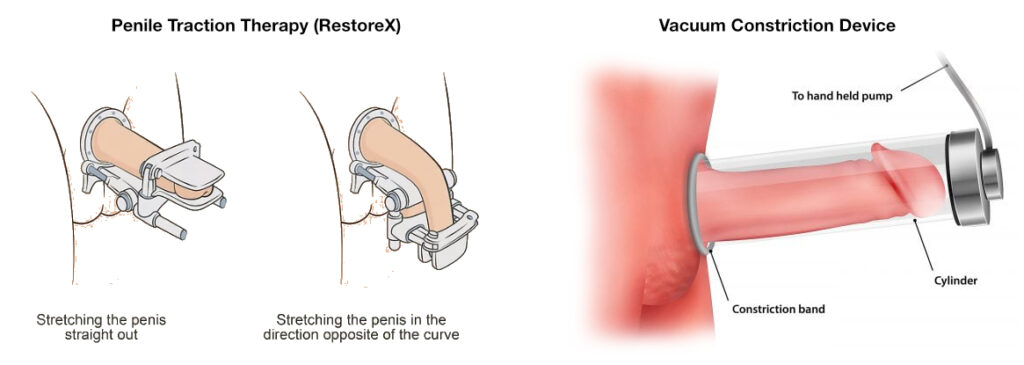
Physical and Mechanical Therapies
Penile traction therapy utilizes a device that applies gradual mechanical tension to the penile shaft to stretch and straighten the penis over time. Vacuum erection devices are used primarily for erectile dysfunction but may also help reduce deformity and improve length in selected cases.
The correct question is rarely "What is the best treatment?" It is "What phase is the disease in, and what function are we trying to preserve?"
Table 2. Comparison of non-surgical treatments
| Treatment | Primary Mechanism | AUA/EAU Recommendation | Reported Efficacy | Key Side Effects/Limitations |
|---|---|---|---|---|
| Collagenase (CCH) | Breaks down collagen in plaque. | AUA: Moderate B. EAU: approved by FDA, but not EMA. | Mean curvature reduction of 38 percent (23 degrees). Overall improvement in 70 percent of men. | Pain, bruising, swelling, hematoma. Rare but serious risk of corporal rupture. Requires strict patient compliance. |
| Intralesional Verapamil | Off-label use; theorized to inhibit fibroblast proliferation. | AUA: Conditional C. EAU: not explicitly recommended, but on list of treatments. | Modest curvature improvement in some patients. | Subjective decreases in curvature and narrowing in some patients. Mild swelling, bruising, and penile pain. |
| Penile Traction Therapy (PTT) | Mechanical force remodels collagen and stretches tissue. | AUA: not specified, but PTT in general is noted. EAU: use to reduce deformity and increase length. | Increases penile length and reduces curvature. Up to 25 percent improvement in curvature for motivated patients. | Requires high patient compliance, often 4-9 hours per day for months. |
| Low-Intensity Shockwave Therapy (LiESWT) | Reduces pain, may disturb pain receptors and increase vascularity. | AUA: Conditional C for pain. EAU: do not use for curvature or plaque size. | Shown to reduce penile pain. No significant benefit on curvature or plaque size. Mixed clinical outcomes for primary goals. | Mixed results and not a primary corrective therapy for deformity. |
Surgical Intervention
For patients with a stable, functional penile deformity, surgery remains the most effective and reliable treatment option and is often considered the gold standard. Surgical intervention is indicated only after the disease has been stable for at least three to six months and when the deformity prevents or significantly complicates sexual intercourse.
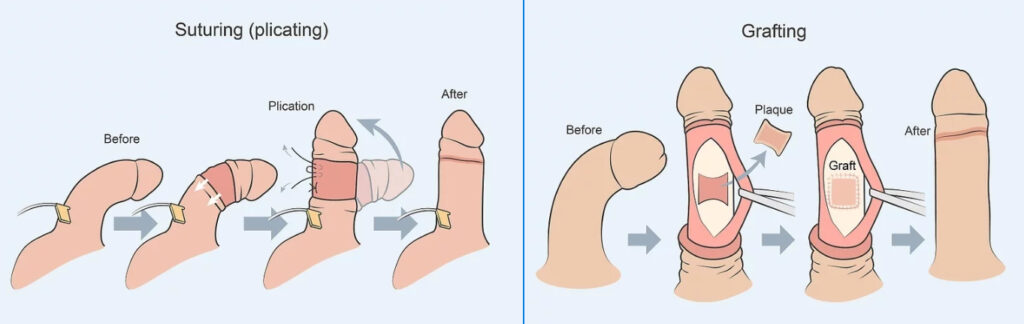
Tunical Plication Procedures
Tunical plication is the first-line surgical option for patients with adequate penile length and a curvature of less than 60 degrees, as well as an absence of complex deformities like an hourglass shape.
Plaque Incision/Excision with Grafting
For patients with more severe deformities, such as a curvature greater than 60 degrees or complex deformities like an hourglass narrowing, plaque incision or excision with grafting is the preferred surgical option.
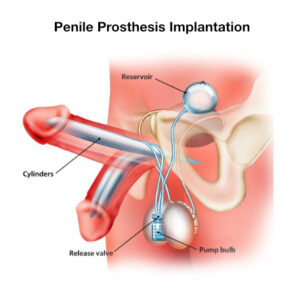
Penile Prosthesis Implantation
The use of a penile prosthesis is the recommended treatment for patients with Peyronie's disease who also have erectile dysfunction that is unresponsive to other therapies.
| Surgical Treatment | Best Indication | Expected Strength | Main Tradeoff or Risk |
|---|---|---|---|
| Tunical Plication | Moderate curvature under 60 degrees with adequate penile length and no major complex deformity. | Highly reliable curvature correction with strong functional outcomes. | Usually perceived penile shortening. |
| Plaque Incision/Excision with Grafting | Curvature over 60 degrees, hourglass deformity, or cases where length preservation matters. | Can correct severe or complex deformity while preserving more length. | Higher risk of postoperative erectile dysfunction. |
| Penile Prosthesis | Peyronie's disease with erectile dysfunction that is unresponsive to other therapies. | Addresses both deformity and erectile rigidity in one procedure with high satisfaction. | Reserved for patients who truly need a prosthesis-based solution. |
Emerging and Experimental Therapies
Low-Intensity Shockwave Therapy (LiESWT)
Low-Intensity Extracorporeal Shockwave Therapy has garnered interest for its potential to treat PD. While it may have a role in reducing pain, it has not been validated as a primary therapy for correcting curvature or reducing plaque size.

Stem Cell Therapy
Stem cell therapy represents a potentially transformative approach to treating PD by targeting the underlying biological mechanisms rather than just the symptoms. It remains experimental, but preliminary work has been promising enough to keep it on the clinical horizon.
The decision tree becomes much clearer once disease phase, erectile function, curvature severity, and length priorities are separated instead of lumped together.
A Practical Clinical Decision-Making Algorithm
The selection of a treatment modality for Peyronie's disease is a complex process that requires careful consideration of the patient's individual clinical profile and expectations. A systematic, step-by-step algorithm is essential for guiding this decision, moving from disease staging to the selection of the most appropriate therapy.
| Treatment Modality | EAU Guideline Recommendation (LE/GR) | AUA Guideline Recommendation (LE/GR) |
|---|---|---|
| Oral Therapies | Do not recommend: Vitamin E, tamoxifen (2b/B); others (3/C). | Conditional recommendation for pentoxifylline (C); others unproven. |
| Intralesional CCH | FDA-approved, not EMA-approved. | Moderate recommendation (B) for curvature 30-90 degrees. |
| Intralesional Verapamil/Interferon | Listed, but no specific recommendation grade. | Conditional recommendation (C). |
| LiESWT | Do not use for curvature or plaque (1b/C). | Conditional recommendation (C) for pain only. |
| PTT/VEDs | Use to reduce deformity and increase length (2b/C). | AUA recommends traction devices, but not VEDs. |
| Surgical Timing | Only when stable for at least 3 months, typically 12 months after onset (3/C). | Surgery only for stable disease. |
| Plication | First option for < 60 degrees curvature with adequate length (2b/B). | Moderate recommendation (C) for patients with adequate rigidity. |
| Grafting | For > 60 degrees curvature, inadequate length, or complex deformities (2b/B). | Moderate recommendation (C) for patients with adequate rigidity. |
| Prosthesis | For patients with concurrent ED (2b/B). | Moderate recommendation (C) for patients with ED. |
Conclusion: Summary and Future Directions
The treatment of Peyronie's disease has advanced significantly from a period of unproven therapies to a structured, evidence-based algorithm. While a complete cure that returns the penis to its pre-disease state remains elusive, the available interventions can effectively manage the condition and restore function and quality of life for almost every patient.
The future of PD management lies in further refining this evidence-based algorithm, personalizing treatment, and continuing to explore new avenues for therapeutic intervention.