Understanding Peyronie’s Disease & Treatment Options
Introduction: Contextualizing the Disease
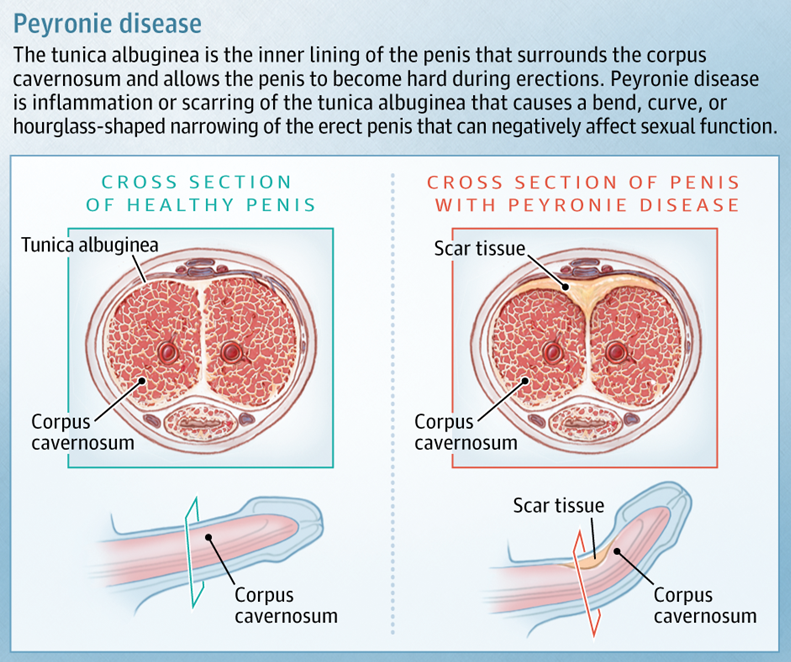
Peyronie’s disease (PD) is a distinct urological condition characterized by the formation of fibrous scar tissue, known as plaque, within the tunica albuginea of the penis. This plaque, which is fundamentally different from arterial or dental plaque, interferes with the elasticity of the penile tissue, leading to a bent or curved erection, penile pain, and potential shortening. The disease is classified as a wound-healing disorder, a categorization that aligns it with other fibrotic conditions like keloids and Dupuytren’s contracture, the latter of which is a thick cord under the skin of the palm that pulls the fingers inward and is often a co-morbid condition. While PD is most prevalent in men aged 40 to 70, its exact epidemiology remains limited.
The precise etiology of PD is not fully understood, but it is believed to be the result of a multifaceted process. The most widely accepted theory posits that repetitive micro-trauma or injury to the penis, often occurring during vigorous sexual activity, triggers an aberrant wound-healing response. However, a significant number of patients cannot recall a specific traumatic event. Other contributing factors include a genetic predisposition, as evidenced by a higher risk in individuals with a family history of the disease, as well as a link to autoimmune and connective tissue disorders such as lupus and Dupuytren’s contracture.
The impact of PD extends far beyond its physical manifestations. The condition can lead to significant psychological and emotional distress, including stress, anxiety, and depression, with some reports indicating that as many as 77% of men with the disease experience notable psychological effects. This profound effect on quality of life and personal relationships underscores the importance of a holistic approach to treatment that considers not only anatomical correction but also the restoration of sexual function and psychological well-being.
Although first observed in 1561 by Fallopius and Vesalius, it was not until 1743 that the disease was fully described by Francois Gigot de la Peyronie, who first depicted an induration of the penis resulting in penile curvature.

The Biphasic Clinical Course: Active vs. Stable Disease
A fundamental principle in the management of PD is the distinction between its two clinical phases: the active inflammatory phase and the chronic stable phase. This biphasic nature is the most critical factor in determining the appropriate treatment strategy. The active phase, which can last for up to 18 months, is characterized by dynamic and changing symptoms, including pain with or without erection, and a gradual worsening of the penile curvature. The pain typically subsides within one to two years, but the physical deformities often persist.
Following the active phase, the disease transitions into the stable phase. This stage is clinically defined by the resolution of pain and the stabilization of the penile curvature and plaque size for a minimum of three to six months. It is only after the disease has reached this stable state that surgical intervention is considered. Non-surgical therapies, by contrast, are often initiated during the active phase with the aim of preventing disease progression and mitigating pain. This clear separation of treatment strategies based on disease phase is foundational to modern clinical practice and is a central theme of this review.
Table 1: Peyronie’s Disease: Staging and Corresponding Management Strategies

Diagnostic Evaluation: Laying the Clinical Foundation
A thorough diagnostic evaluation is essential for effective management of Peyronie’s disease. The initial assessment begins with a focused medical and sexual history, which should include the duration of symptoms, the presence and severity of penile pain, the degree and direction of deformity, and any associated erectile dysfunction (ED). This historical information is sufficient to establish a diagnosis in most cases. A physical examination of the genitalia is also mandatory to palpate for the presence of a fibrous plaque and to assess for related conditions, such as Dupuytren’s contracture or Ledderhose disease of the plantar fascia.

For a definitive and objective assessment of the penile curvature, a measurement of the erect penis is crucial. While a pharmacologically induced erection in a clinical setting via intracavernous injection (ICI) is considered a superior method for an objective assessment, the use of a patient’s self-photograph of a natural erection is also a widely accepted and mandatory method for documenting the deformity. This reliance on patient-provided self-documentation as a valid clinical metric highlights a pragmatic approach to diagnosis, recognizing that it can provide an accurate assessment without the need for an invasive office procedure. Ultrasound, a non-invasive tool, can also be used to visualize the plaque and assess penile hemodynamics, but major guidelines do not recommend it for routine measurement of plaque size.
Non-Surgical Treatment Modalities: Management of Active and Chronic Disease
A variety of non-surgical treatments are available for Peyronie’s disease, with the most appropriate option depending heavily on the disease stage and patient-specific factors.
Oral Therapies
Historically, numerous oral agents have been used to treat PD, but a shift towards evidence-based practice has led to a re-evaluation of their efficacy. Major clinical guidelines, including those from the European Association of Urology (EAU) and the American Urological Association (AUA), largely do not recommend oral therapies for the significant reduction of penile curvature or plaque size. Specifically, agents such as vitamin E, tamoxifen, procarbazine, and omega-3 fatty acids are considered to have a lack of proven efficacy. While some studies have suggested a benefit from pentoxifylline in the active stage, the AUA guideline offers only a conditional recommendation for its use, citing limited and conflicting evidence. There have also been suggestions that daily phosphodiesterase type-5 inhibitors (PDE5Is), such as tadalafil, may result in the resolution of septal scar tissue, though this remains an area of limited evidence. This prevailing clinical consensus highlights the move away from historical, unproven practices toward a more rigorous, data-driven approach.
Intralesional Injection Therapy
Intralesional injections involve the direct administration of a therapeutic agent into the penile plaque, offering a more targeted approach than systemic oral medications.
Collagenase Clostridium Histolyticum (CCH) – XIAFLEX
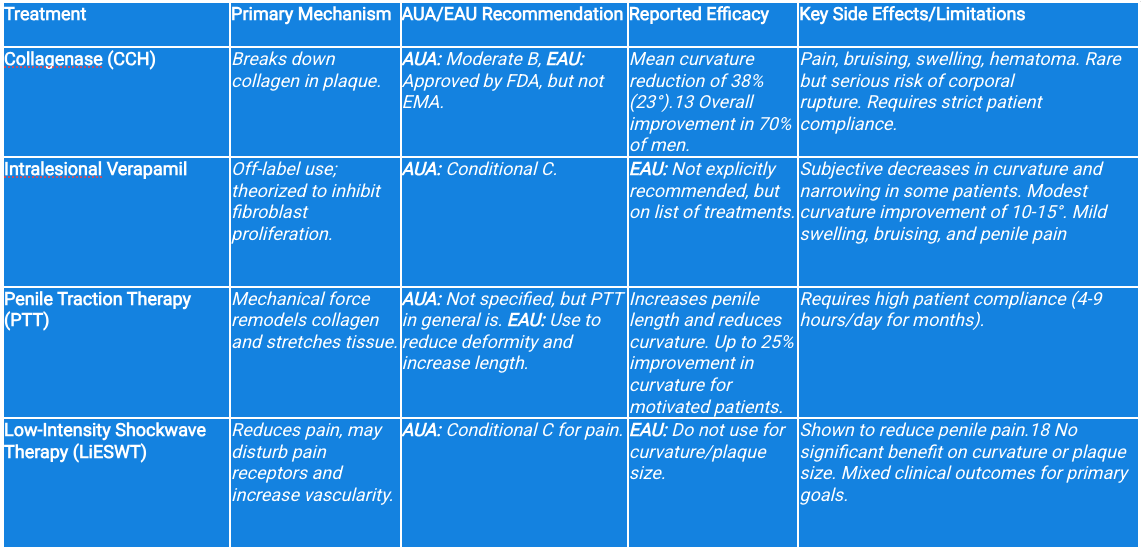
Collagenase Clostridium histolyticum (CCH), marketed as XIAFLEX, is the only drug approved by the U.S. Food and Drug Administration (FDA) for the treatment of PD. It is indicated for men with a palpable plaque and a penile curvature between 30 and 90 degrees. The mechanism of action involves the direct enzymatic breakdown of the collagen that constitutes the fibrous plaque, thereby reducing the penile bend. Clinical trials have demonstrated modest yet significant efficacy, with a mean curvature reduction of 23 degrees, representing an average improvement of 38%. Overall, CCH treatment, when combined with patient-administered penile modeling, is reported to result in improvement for 70% of men.
Treatment with CCH is a multi-step protocol that necessitates significant patient compliance. A typical treatment cycle consists of two injections spaced a few days apart, followed by at-home penile modeling exercises. This cycle may be repeated up to four times. A crucial component of the treatment protocol is the requirement to abstain from sexual activity for a minimum of four weeks after the second injection of a cycle to mitigate the risk of adverse events. Common side effects include localized pain, bruising, swelling, and hematoma. The most serious, albeit rare, complication is corporal rupture, or “penile fracture,” which can occur during vigorous intercourse or even a spontaneous erection. This underscores the necessity of comprehensive patient counseling regarding the risks and the importance of strict adherence to the post-injection activity restrictions.

Verapamil and Interferon-α2b
Other intralesional agents, such as verapamil and interferon-α2b, are considered “off-label” treatments for PD. Verapamil, a calcium channel blocker, has been anecdotally reported to decrease penile narrowing and curvature, and its side effects are generally mild, including temporary pain and bruising. Interferon-α2b has shown promise in some studies, leading to significant reductions in mean curvature and plaque size, particularly in patients with smaller plaques. However, other studies have found it to be less effective and associated with bothersome side effects, such as flu-like symptoms, which can lead to treatment discontinuation. The AUA guideline offers only a conditional recommendation for both of these agents, noting the conflicting evidence and limited data. This continued use of off-label therapies highlights the need for more high-quality, non-industry-supported research to definitively establish their role in the treatment paradigm.

Physical and Mechanical Therapies
Physical and mechanical therapies offer a non-pharmacological approach to improving penile deformity and length.
Penile Traction Therapy (PTT)
Penile traction therapy (PTT) utilizes a device that applies gradual mechanical tension to the penile shaft to stretch and straighten the penis over time. The proposed mechanism is “mechanotransduction,” a process that stimulates cellular biochemical responses to mechanical stress, leading to the remodeling of collagen fibers and expansion of the extracellular matrix. Studies on PTT have shown promising results, with some reports indicating a significant increase in penile length and a reduction in curvature. For example, one small study found a 14-degree decrease in mean curvature and a 4.1 cm increase in mean penile length. However, the effectiveness of PTT is directly linked to patient motivation and compliance, as it requires daily use for several hours over a period of months. This reliance on consistent, long-term patient effort is a key determinant of its real-world success. The only device approved by the FDA is RestoreX.
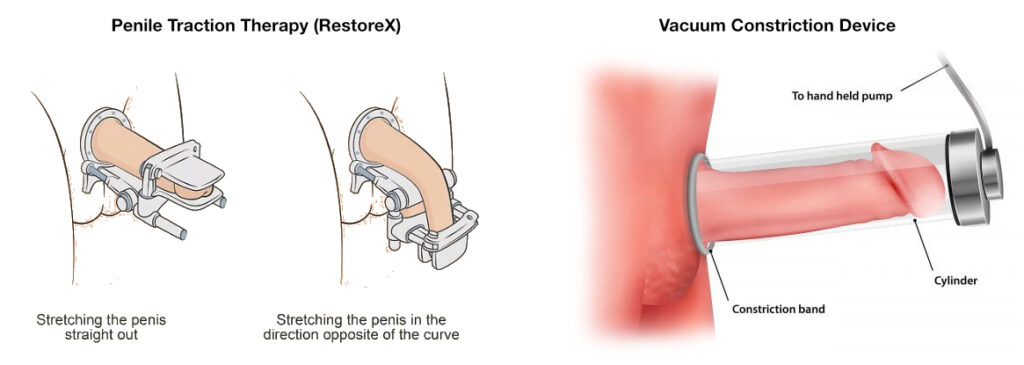
Vacuum Erection Devices (VEDs)
Vacuum erection devices (VEDs) are used primarily for the treatment of erectile dysfunction but have also been shown to be beneficial in PD for reducing penile deformity and increasing penile length. While they can be used as a stand-alone therapy, they are explicitly contraindicated during treatment with CCH due to the potential for increased bleeding. This highlights the need for a coordinated treatment plan to prevent complications from overlapping therapies.
Table 2: Comparison of Non-Surgical Treatments for Chronic Peyronie’s Disease
Surgical Intervention
For patients with a stable, functional penile deformity, surgery remains the most effective and reliable treatment option, and is often considered the gold standard. Surgical intervention is indicated only after the disease has been stable for at least three to six months and when the deformity prevents or significantly complicates sexual intercourse. Prior to surgery, a comprehensive assessment of penile length, curvature severity, erectile function, and patient expectations is mandatory.
Surgical Techniques
The choice of surgical procedure is dictated by the patient’s unique clinical profile, including the degree of curvature, presence of ED, and penile length.
Tunical Plication Procedures
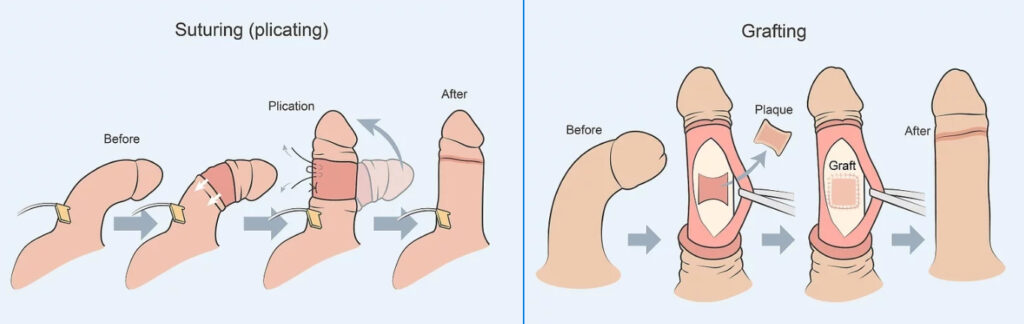
Tunical plication is a tunical shortening procedure that involves placing sutures on the side of the penis opposite to the curve to effectively straighten it. It is the first-line surgical option for patients with adequate penile length and a curvature of less than 60 degrees, as well as an absence of complex deformities like an hourglass shape.8 The outcomes of plication are highly favorable, with one study reporting that 96% of patients had improved curvature and 93% were able to achieve an erection adequate for sexual intercourse.19 The primary drawback of this procedure is the almost universal experience of perceived penile shortening, a trade-off that patients must be willing to accept in exchange for reliable and permanent curvature correction. The success of this technique relies heavily on managing patient expectations and ensuring they are prepared for this outcome.
Plaque Incision/Excision with Grafting
For patients with more severe deformities, such as a curvature greater than 60 degrees or complex deformities like an hourglass narrowing, plaque incision or excision with grafting is the preferred surgical option. This tunical lengthening procedure involves surgically incising or excising the plaque and covering the resulting defect with a graft. The technique can restore length and correct both the curvature and complex narrowing. Success rates are high, ranging from 75% to over 90%.20 The major risk, however, is the potential for worsening or developing new erectile dysfunction, which can occur in 10-50% of men postoperatively. For this reason, grafting is typically reserved for men with excellent pre-operative erectile function.
Penile Prosthesis Implantation
The use of a penile prosthesis is the recommended treatment for patients with Peyronie’s disease who also have erectile dysfunction that is unresponsive to other therapies. A prosthesis simultaneously corrects the penile curvature and provides a functionally rigid erection, making it a highly effective single-stage solution for this patient population. Penile prostheses have the highest rate of patient and partner satisfaction of all available ED treatments. In cases where significant deformity persists after the prosthesis is inserted, adjunctive procedures such as modeling, plication, or grafting can be performed intra-operatively.
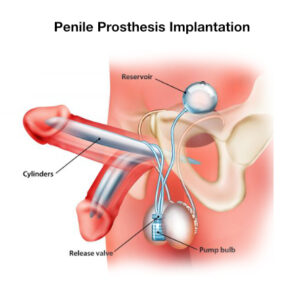
Table 3: Surgical Treatments for Peyronie’s Disease: Indications, Outcomes, and Risks
Emerging and Experimental Therapies
The field of Peyronie’s disease treatment continues to evolve, with new and experimental therapies being investigated to address the limitations of current options.
Low-Intensity Shockwave Therapy (LiESWT)
Low-Intensity Extracorporeal Shockwave Therapy (LiESWT) has garnered interest for its potential to treat PD. While some initial meta-analyses suggested it could reduce penile pain and improve sexual function, the clinical outcomes for curvature correction and plaque size reduction have been largely mixed. Major clinical guidelines have since weighed in, with the EAU explicitly stating that LiESWT should not be used to improve penile curvature or reduce plaque size. The AUA also does not recommend it for curvature reduction but conditionally recommends it for the reduction of penile pain. This divergence highlights a crucial distinction: while LiESWT may have a role in managing a single symptom (pain) in the active phase, it has not been validated as a primary therapy for correcting the underlying deformity.

Stem Cell Therapy
Stem cell therapy represents a potentially transformative approach to treating PD by targeting the underlying biological mechanisms rather than just the symptoms. Preliminary research, primarily in animal models, has shown promising results. Adipose-derived stem cells (ADSCs), due to their accessibility and anti-inflammatory properties, are being investigated for their ability to promote tissue repair and prevent the fibrotic process. While still in the experimental stage, this approach has the potential to fundamentally alter the disease course, moving from a paradigm of managing the scar to one of preventing its formation entirely.
A Practical Clinical Decision-Making Algorithm
The selection of a treatment modality for Peyronie’s disease is a complex process that requires careful consideration of the patient’s individual clinical profile and expectations. A systematic, step-by-step algorithm is essential for guiding this decision, moving from disease staging to the selection of the most appropriate therapy.
The first step involves a crucial determination of the disease’s stage. If the patient is in the active, inflammatory phase, the focus should be on observation, pain management, and the potential use of intralesional injections or penile traction therapy to mitigate the worsening of the curvature. Surgical intervention is strictly contraindicated during this period.
Once the disease has entered the stable phase, the next consideration is the patient’s erectile function. If the patient has ED that does not respond to oral medications or other less invasive therapies, a penile prosthesis is the most effective and direct solution. This option addresses both the curvature and the erectile dysfunction in a single procedure.
For patients in the stable phase who have preserved erectile function, the decision is guided by the severity of the curvature and patient preference for length preservation. For a moderate curvature (less than 60 degrees) and adequate penile length, non-surgical options like CCH or PTT can be offered. Alternatively, a tunical plication procedure can provide a reliable surgical correction. For severe curvatures (greater than 60 degrees) or complex deformities, which often require a length-preserving approach, a plaque incision/excision with grafting is the recommended surgical option.
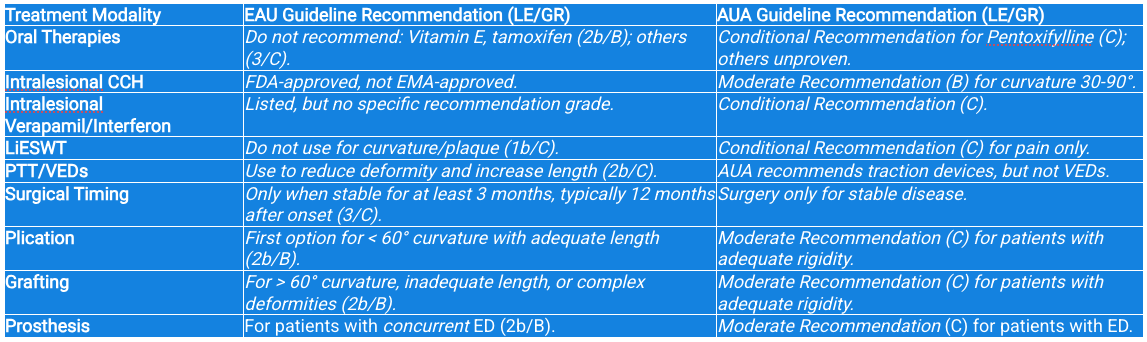
Table 4: Summary of Major Clinical Guidelines (AUA vs. EAU)
Conclusion: Summary and Future Directions
The treatment of Peyronie’s disease has advanced significantly from a period of unproven therapies to a structured, evidence-based algorithm. While a complete “cure” that returns the penis to its pre-disease state remains elusive, the comprehensive range of available interventions can effectively manage the condition and restore function and quality of life for almost every patient.
For a patient in the active phase, a conservative approach centered on observation and pain management is recommended. Once the disease has stabilized, the choice between non-surgical and surgical options depends on the specific patient profile. Collagenase Clostridium histolyticum is the only FDA-approved non-surgical option with proven efficacy, but its use is part of a complex, patient-dependent protocol. Penile traction therapy also offers a viable non-invasive option, although its success is highly correlated with patient commitment.
For stable disease, surgical intervention provides the most reliable and definitive results. Plication is the ideal choice for moderate curvatures, offering a high success rate in exchange for some degree of length loss. Grafting is a more complex procedure reserved for severe curvatures and aims to preserve length, though it carries a higher risk of postoperative erectile dysfunction. The penile prosthesis is the most definitive solution for patients with concurrent ED, effectively addressing both the deformity and the functional impairment in a single, highly satisfying procedure.
The current guidelines highlight a clear consensus on surgical approaches, but there remains a need for more high-quality, non-industry-supported research on non-surgical and emerging therapies. Continued investigation into therapies like stem cell therapy, which targets the underlying biological process, may eventually lead to a more fundamental and less invasive “cure” for this complex and challenging disease. The future of PD management lies in further refining this evidence-based algorithm, personalizing treatment, and continuing to explore new avenues for therapeutic intervention.

Author
Dr Arno Kroner
OMD LAc IFMCP
References
- Peyronie’s disease – Symptoms and causes – Mayo Clinic, accessed August 29, 2025, https://www.mayoclinic.org/diseases-conditions/peyronies-disease/symptoms-causes/syc-20353468
- Peyronie’s Disease – Symptoms and Causes | Penn Medicine, accessed August 29, 2025, https://www.pennmedicine.org/conditions/peyronies-disease
- Peyronie’s disease – Watch out for the bend – RACGP, accessed August 29, 2025, https://www.racgp.org.au/afp/2017/september/peyronies-disease
- 8. penile curvature – EAU Guidelines on Sexual and Reproductive Health – Uroweb, accessed August 29, 2025, https://uroweb.org/guidelines/sexual-and-reproductive-health/chapter/penile-curvature
- Intralesional interferon-alpha-2b for the treatment of Peyronie’s disease – Dupuytren Research Group, accessed August 29, 2025, https://dupuytrens.org/DupPDFs/2002_Lacy.pdf
- Peyronie’s Disease: AUA Guideline – PMC, accessed August 29, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC5027990/
- Treating Your Peyronie’s Disease with Male Prosthetics – Arizona Urology, accessed August 29, 2025, https://www.arizona-urology.com/blog/treating-your-peyronies-disease-with-male-prosthetics
- EAU GUIDELINES ON PENILE CURVATURE – Cloudfront.net, accessed August 29, 2025, https://d56bochluxqnz.cloudfront.net/media/Penile-curvature-2017-pocket.pdf
- Peyronie’s Disease, Treatment, Causes, & Symptoms | University of Utah Health, accessed August 29, 2025, https://healthcare.utah.edu/mens-health/conditions/peyronies
- EAU guidelines on penile curvature – PubMed, accessed August 29, 2025, https://pubmed.ncbi.nlm.nih.gov/22658761/
- Xiaflex: A New Treatment for Peyronie’s Disease – Premier Medical Group, accessed August 29, 2025, https://www.premiermedicalhv.com/news/xiaflex-new-treatment-peyronies-disease/
- Treatment of Peyronie’s Disease < Sexual and Reproductive Medicine Blog, accessed August 29, 2025, https://medicine.yale.edu/lab/urology-mens-health-blog/2022/mar/
- Complications and other concerns with intralesional injection therapy with collagenase clostridium histolyticum for Peyronie’s disease, accessed August 29, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC5313307/
- Possible Side Effects – XIAFLEX for Peyronie’s disease, accessed August 29, 2025, https://peyronies-disease.xiaflex.com/patient/xiaflex/side-effects/
- Intralesional Injection Therapies for Peyronie’s Disease | San Diego Sexual Medicine, accessed August 29, 2025, https://www.sdsm.info/male-treatments/intralesional-injection-therapies-for-peyronies-disease
- Penile traction therapy for Peyronie’s disease—what’s the evidence? – Usta, accessed August 29, 2025, https://tau.amegroups.org/article/view/9817/html
- Penile traction therapy and Peyronie’s disease: a state of art review of the current literature, accessed August 29, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC3547530/
- Pro: does shockwave therapy have a place in the treatment of Peyronie’s disease?, accessed August 29, 2025, https://tau.amegroups.org/article/view/10269/html
- Favorable Patient Reported Outcomes After Penile Plication for Wide Array of Peyronie Disease Abnormalities – Dr. Allen Morey, accessed August 29, 2025, https://drallenmorey.com/wp-content/uploads/2023/04/Favorable-Patient-Reported-Outcomes.pdf
- Plaque Incision or Excision with Grafting for Treatment of Peyronie’s Disease – New York Urology Specialists, accessed August 29, 2025, https://www.newyorkurologyspecialists.com/peyronies/plaque-excision/
- Grafting (penile lengthening) surgical techniques – International Andrology London, accessed August 29, 2025, https://london-andrology.co.uk/uro-genital-health/peyronies-disease/grafting-penile-lengthening-surgical-techniques/
- Penile implants – Mayo Clinic, accessed August 29, 2025, https://www.mayoclinic.org/tests-procedures/penile-implants/about/pac-20384916
- Advances in stem cell therapy for the treatment of Peyronie’s disease – PMC, accessed August 29, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC7062597/