Chronic Kidney Disease and Functional Medicine – Exploring Integrative Approaches
Chronic Kidney Disease (CKD) is no longer a niche medical concern; it is a global epidemic. Currently, over 850 million people worldwide—roughly 10% of the global population—are living with kidney disease. In the United States and Europe, the statistics are strikingly similar: approximately 1 in 7 adults is affected, though a staggering 90% of them remain undiagnosed until the later stages. (International Society of Nephrology (ISN) and the American Society of Nephrology (ASN). The WHO now classifies kidney disease as the 9th or 10th leading cause of death globally (up from 13th just a few years ago).
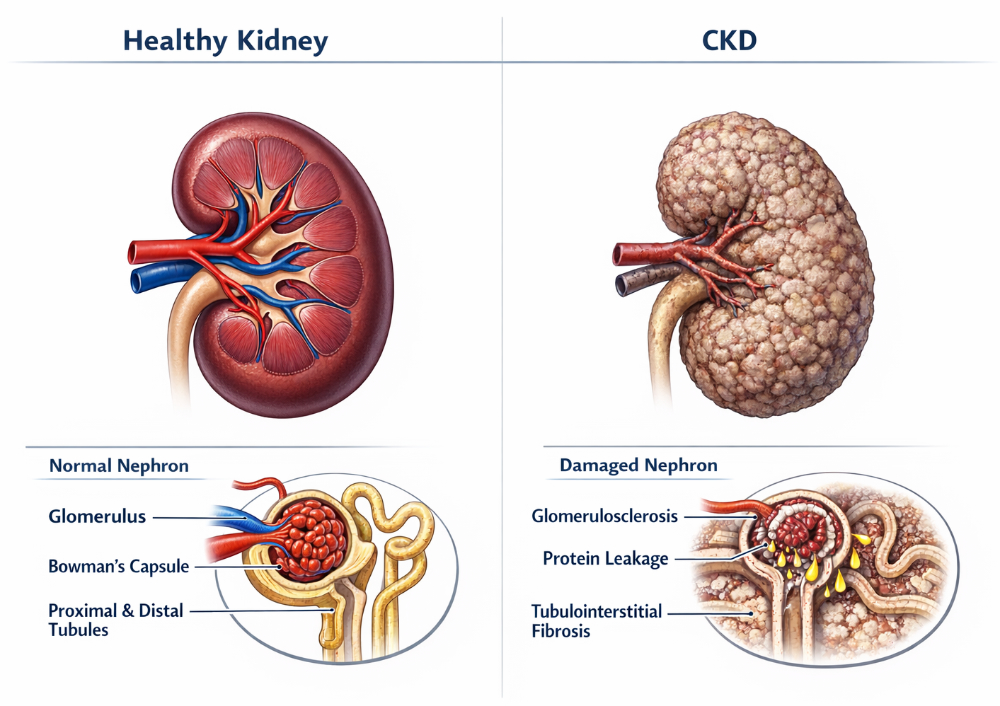
What is Chronic Kidney Disease (CKD)?
Think of the kidneys as the body’s master chemical engineers, not just passive filters. Imagine a high-tech filtration plant in the home that cleans the water, balances minerals, regulates water pressure, and signals the heater when to engage. Chronic Kidney Disease is the slow, silent decline of that plant. Over years, as the “filters” lose their efficiency, metabolic waste begins to back up, physically damaging the “pipes” (blood vessels) and polluting the body’s internal environment.
Why It Matters: The Systemic Ripple Effect
When the kidneys struggle, the impact is felt far beyond the renal system. As the internal chemistry becomes unbalanced, the “backlog” triggers a cascade of failures across the body:
- The Energy Crash: The buildup of “metabolic trash” poisons the cellular engines, leading to profound, bone-deep exhaustion.
- The Cardiovascular Strain: Imbalances in fluid and minerals act like high-pressure surges in the plumbing, straining the heart and stiffening the arteries.
- The Structural Shift: The kidneys stop activating the hormones that maintain bone density, leading the body to “strip the skeleton for parts.”
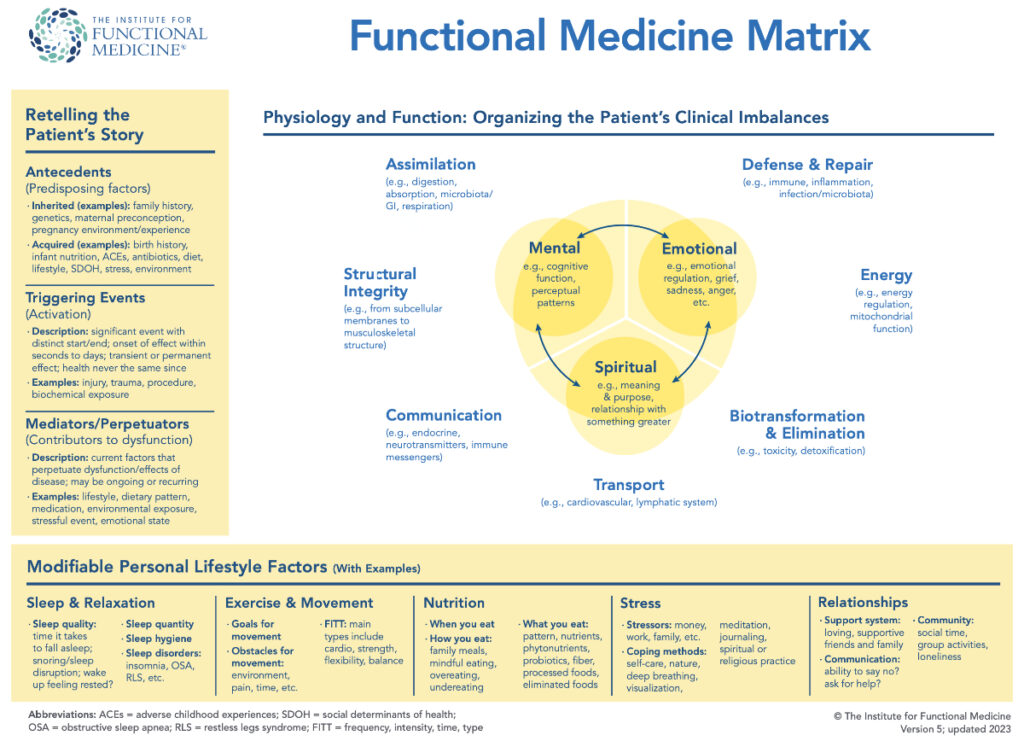
The Functional Medicine Perspective: The Matrix
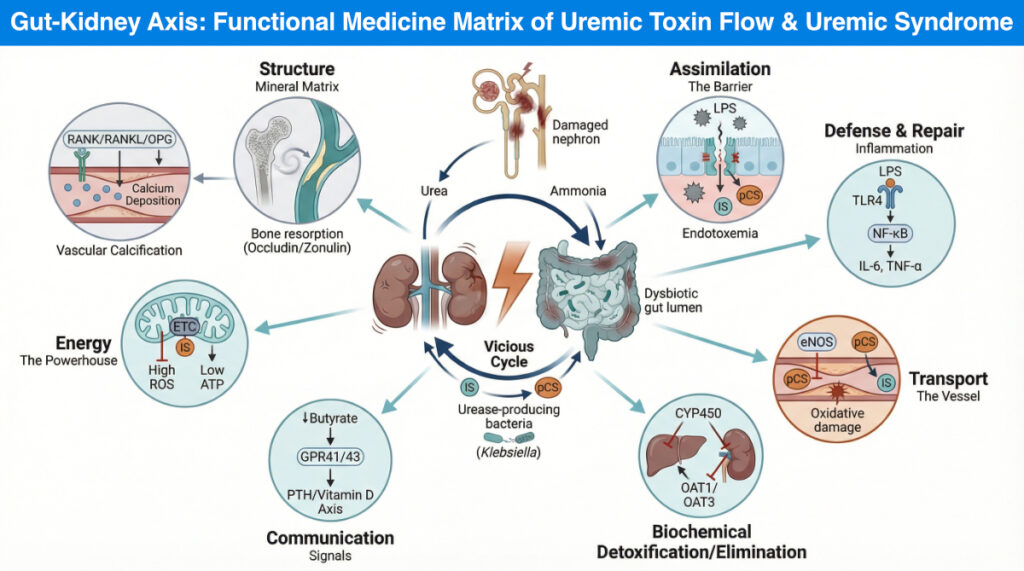
In Functional Medicine, we don’t see CKD as an isolated organ failure; we see it as a disruption in a dynamic, interconnected web. We use the IFM Matrix—a clinical roadmap—to look past the “kidney” label and identify the root causes. By mapping health across seven physiological nodes—like Assimilation, Energy, and Detoxification—we can see how a “clog” in one system creates ripples of dysfunction across the entire map. This allows us to move from simply managing a diagnosis to restoring the biological balance of the whole person.
When we apply this systems-biology lens to Chronic Kidney Disease (CKD), we stop seeing the kidney as a failing filter in a vacuum. Instead, we begin to uncover a “toxic dialogue” between the gut and the kidneys, where imbalances in the microbiome (dysbiosis) trigger a cascade of inflammation and metabolic gridlock that impacts every node of the matrix. This approach allows us to move from simply managing a diagnosis to addressing the systemic root causes of the disease.
The Gut-Kidney-Body Connection
1. Assimilation – The Entry Point of the “Toxic Dialogue”
In the Functional Medicine Matrix, Assimilation covers how we take the outside world and bring it into our internal environment. In a healthy state, the gut is a selective gatekeeper. In CKD, however, this gatekeeper is compromised by a process called Uremic Dysbiosis.
- The Biochemical “Why”: As kidney function declines, the body can no longer clear urea through the urine. To compensate, the body shunts this urea into the gastrointestinal tract. Here, specific bacteria containing the enzyme urease break that urea down into ammonia (NH₃) and ammonium hydroxide (NH₄OH).
- The Breakdown: This ammonia spike raises the local pH of the gut, which acts like a “chemical burn” on the intestinal lining. This dissolves the Tight Junction proteins (Zonulin and Occludin) that keep the gut wall sealed. The result is increased intestinal permeability (IP), commonly known as “Leaky Gut.” – When I perform a stool test I always measure Zonulin levels.
- The Resulting Flux: Instead of absorbing life-sustaining nutrients, the body begins “assimilating” dangerous cargo:
- Lipopolysaccharides (LPS): Pro-inflammatory fragments of bacterial cell walls.
- Uremic Toxins: Compounds like Indoxyl Sulfate and p-Cresol Sulfate that are fermented by “bad” bacteria in this high-ammonia environment.
- The Systemic Impact: This creates a constant, low-grade “drip” of endotoxins directly into the portal circulation, forcing the liver and the immune system to deal with a burden they were never meant to carry.
2. Defense and Repair – The Immune Response
In the IFM Matrix, Defense and Repair focuses on the immune system and the inflammatory response. In a Stage 4 CKD patient, this node is stuck in a state of “perpetual alarm.” Because the Assimilation node has failed, the immune system is forced to deal with a constant influx of invaders it was never designed to handle 24/7.
When the gut barrier breaks down, the “messengers of decay” (LPS and uremic toxins) enter the bloodstream. This is where the immune system—the primary defense—becomes a driver of the disease itself through a process called Systemic Chronic Inflammation.
- The Biochemical “Why”: Once in the blood, LPS binds to a specific sensor on immune cells called Toll-Like Receptor 4 (TLR4).
- The Breakdown: Think of TLR4 as a “tripwire.” When LPS hits it, it triggers a master genetic switch called NF-κB. Once flipped, this switch tells DNA to start mass-producing pro-inflammatory cytokines like IL-6, TNF-α, and IL-1β.
- The Resulting Damage: In a healthy person, this response turns off once the threat is gone. In CKD, the “leaky gut” ensures the threat never goes away. This constant cytokine storm leads to:
- Renal Fibrosis: The immune system tries to “repair” the kidney by laying down scar tissue, which unfortunately further destroys the remaining healthy nephrons.
- Immune Exhaustion: This is why CKD patients are often more susceptible to outside infections; their “Defense” system is too busy fighting the gut-derived “fire” to notice a new virus or bacteria.
3. Transport – The Delivery System
This node is often the most critical for CKD patients, as cardiovascular complications are the leading systemic risk in kidney disease. The “Transport” system is responsible for moving nutrients and oxygen, but in the presence of gut dysbiosis, it becomes a delivery vehicle for uremic toxins.
- The Biochemical “Why”: The spotlight here is on eNOS (endothelial Nitric Oxide Synthase). In a healthy vessel, eNOS produces Nitric Oxide (NO), a gas that tells blood vessels to relax, dilate, and stay flexible.
- The Breakdown (eNOS Uncoupling): Uremic toxins, specifically Indoxyl Sulfate, create an environment of intense oxidative stress. This causes a phenomenon called “eNOS uncoupling.” Think of it like a gear slipping in a machine: instead of producing helpful Nitric Oxide, the “uncoupled” enzyme starts producing Superoxide (O-2), a highly reactive and damaging free radical.
- The Resulting Damage:
- Endothelial Dysfunction: Without Nitric Oxide, blood vessels become stiff and unable to dilate. This drives up blood pressure and places immense strain on the heart.
- Accelerated Atherosclerosis: The Superoxide produced by uncoupled eNOS “rusts” the lining of the arteries, leading to rapid plaque formation and vascular calcification.
- The Systemic Echo: This is why “kidney issues” so quickly become “heart issues.” The toxins aren’t just passing through; they are physically dismantling the transport system’s ability to regulate blood flow.
4. Biotransformation & Elimination – The Bottleneck
In the IFM Matrix, Biotransformation and Elimination are the two halves of the body’s waste management system. Biotransformation (Phase I and II detoxification) is the chemical processing of toxins, largely in the liver, while Elimination is the physical removal of that waste. In CKD, this system doesn’t just slow down—it experiences a catastrophic industrial backup.
When the kidneys (the primary exit) fail to filter, the body doesn’t just stop producing waste. Instead, the waste backs up into the “processing plant” (the liver).
- The Biochemical “Why”: The spotlight here is on the Cytochrome P450 (CYP450) enzyme system. These enzymes are responsible for metabolizing everything from hormones to 70–80% of all clinical drugs. In CKD, the high levels of circulating uremic toxins (like Indoxyl Sulfate) act as “transcriptional silencers.” They don’t just block the enzymes; they actually send signals to the liver cell’s nucleus to stop producing the CYP450 genes altogether.
- Genetic Silencing: Because the liver is bathing in uremic blood, it downregulates its Phase I and Phase II detoxification pathways.
- Transporter Inhibition: Even the toxins the liver does manage to process can’t leave. Proteins called Organic Anion Transporters (OAT1 and OAT3), which usually ferry toxins into the kidney for disposal, become “clogged” or inhibited by the sheer volume of gut-derived waste.
- The Result – Total Body Burden: This creates a state where the body is literally marinating in its own metabolic trash. This leads to:
- Severe Medication Sensitivity: Drugs that would normally stay in the system for 6 hours might stay for 24, drastically increasing the risk of side effects and toxicity.
- Uremic Pruritus (Itching): When the kidneys and liver can’t clear toxins, the body tries to eliminate them through the skin—the “third kidney”—causing the relentless, deep-seated itching common with late stage CKD.
- Metabolic Encephalopathy: The “backup” reaches the brain, manifesting as profound brain fog, cognitive decline, and irritability.
5. Communication – The Signal Interference
In the IFM Matrix, Communication refers to how cells, tissues, and organs talk to one another via hormones, neurotransmitters, and signaling molecules. In CKD, the gut-kidney axis is like a telephone line filled with static. The “good” signals are lost, and “bad” signals take over, disrupting everything from blood sugar to bone density.
When the gut is in a state of dysbiosis, it stops producing the “peacekeeping” signals the body relies on for stability. Simultaneously, the failing kidney sends out “distress signals” that throw the rest of the endocrine system into disarray.
- The Biochemical “Why” – The Lost Messengers: A healthy gut microbiome ferments fiber into Short-Chain Fatty Acids (SCFAs), primarily Butyrate. Butyrate isn’t just fuel for the gut; it is a powerful signaling molecule that travels to the brain and kidneys to activate G-Protein Coupled Receptors (GPR41 and GPR43).
- The Breakdown: In uremic dysbiosis, butyrate-producing bacteria are killed off. The loss of these signals means:
- Metabolic Miscommunication: Without SCFA signaling, insulin sensitivity drops. This is why many CKD patients struggle with insulin resistance and fluctuating blood sugar, even if they aren’t diabetic.
- Blood Pressure Static: SCFAs help regulate the renin-angiotensin system. When these signals vanish, the body loses a key “braking” mechanism for hypertension.
- The Resulting Hormonal “Crosstalk”: Because the kidneys are struggling, they over-communicate with the parathyroid glands.
- The PTH-Vitamin D Axis: The kidney fails to convert Vitamin D into its active form (1,25(OH)2D). In response, the body pumps out Parathyroid Hormone (PTH).
- The Result: High PTH levels tell the body to “strip the bones for parts” to maintain blood calcium levels.
- The Result – Systemic Static: The patient experiences a body that feels “out of sync.” This communication breakdown manifests as:
- Emotional Fragility: Disrupted gut-brain communication affects serotonin production, contributing to the depression and anxiety common in CKD.
- Secondary Hyperparathyroidism: A state where the “Communication” node is so loud and distorted that it begins to physically dismantle the “Structure” node (the bones).
6. Energy – The Power Grid
In the IFM Matrix, the Energy node is where the “total body burden” of CKD becomes a physical reality for the patient. This node tracks how we transform food and oxygen into the cellular currency of life: ATP. In CKD, the body experiences a systemic power failure because the “mitochondrial engines” are being poisoned by the very waste the body cannot eliminate.
The profound, “bone-deep” fatigue CKD patients feel isn’t just about being tired—it is a cellular inability to produce energy. The kidneys are among the most mitochondria-dense organs in the body; when their power grid fails, the rest of the body follows.
- The Biochemical “Why” – The ETC Blockade: Inside every cell, the Electron Transport Chain (ETC) is a series of molecular “pumps” (Complexes I through IV) that create ATP. Uremic toxins, specifically Indoxyl Sulfate, act as direct mitochondrial poisons. They penetrate the mitochondrial membrane and interfere with Complex I and Complex III, the primary entry points for energy production.
- The Breakdown – Oxidative Leakage: When these complexes are blocked, electrons “leak” out of the chain before they can be turned into ATP. These rogue electrons react with oxygen to create Reactive Oxygen Species (ROS)—highly unstable molecules that damage mitochondrial DNA.
- The Result – A Sputtering Engine:
- Low ATP Production: Like a car engine running on contaminated fuel, the mitochondria “sputters.” The yield of ATP drops significantly, leaving the body in a permanent state of energy bankruptcy.
- Mitochondrial Fission: Under the stress of uremic toxins, mitochondria begin to fragment and die, a process that accelerates muscle wasting (sarcopenia).
- The Systemic Echo: This energy crisis creates a “metabolic trap.”
- Muscle Fatigue: Because the heart and skeletal muscles are energy-hungry, they are the first to suffer. This is why late CKD Stage patients often experience heavy limbs and shortness of breath with minimal exertion.
- Repair Shutdown: Without ATP, the “Defense and Repair” node cannot function. The body literally lacks the “cash” (ATP) to pay for cellular cleanup and tissue repair, leading to the rapid progression of the disease.
7. Structure – The Framework & Mineral Migration
In the IFM Matrix, Structure refers to the physical integrity of the body—from the microscopic architecture of the cell membrane to the macroscopic strength of the skeletal system. In CKD, the structural integrity of the body undergoes a “Mineral Migration”: minerals leave the places they belong (the bones) and settle in the places they don’t (the arteries).
This node is where the “Communication” static and the “Energy” failure manifest as physical damage. The breakdown of the skeleton and the stiffening of the cardiovascular system are the structural hallmarks of advanced kidney disease.
- The Biochemical “Why” – The RANK/RANKL Pathway: Because the kidney can no longer manage phosphorus or activate Vitamin D, the “Communication” node sends a frantic signal via Parathyroid Hormone (PTH). This activates a molecular switch called the RANK/RANKL pathway.
- The Breakdown – Bone-to-Blood Shift: RANKL is a signaling protein that tells the body to “dissolve the bone.” It activates cells called osteoclasts, which chew up the bone matrix to release calcium into the bloodstream.
- The Results:
- Vascular Calcification: This is the ultimate structural irony of CKD. While the bones become porous and brittle (Renal Osteodystrophy), the excess calcium—driven by oxidative stress and uremic toxins—deposits into the soft tissues of the blood vessels.
- The “Crunchy” Artery: Using the Wnt/β-catenin signaling pathway, the smooth muscle cells in the arteries actually “reprogram” themselves to act like bone cells. They begin to lay down a calcium matrix inside the vessel wall.
- The Systemic Echo: The structural failure is two-fold:
- Skeletal Fragility: An increased risk of fractures and chronic bone pain.
- Loss of Vascular Compliance: As arteries turn to “stone,” the heart has to pump against a rigid pipe instead of a flexible tube. This leads to Left Ventricular Hypertrophy (an enlarged, overworked heart) and is a primary driver of heart failure in late stage patients.
Summary Table
|
IFM Node |
The Systemic Impact |
Symptoms |
| Assimilation |
Leaky gut & toxic absorption |
Bloating, food sensitivities |
| Defense |
Chronic systemic inflammation |
Aches, slow healing |
| Transport |
Endothelial (vessel) damage |
High blood pressure, heart issues |
| Detox/Elimination |
Liver/Kidney backup |
Medication side effects, itching |
| Communication | Hormone & SCFA disruption | Blood sugar swings |
| Energy | Mitochondrial “poisoning” |
Crushing fatigue |
| Structure |
Bone loss & arterial stiffness |
Bone pain, “stiff” feeling |
BOOK A FREE DISCOVERY CALL
The Clinical Action Plan: Rebalancing the Matrix
Rather than chasing symptoms, I use targeted interventions to break the “vicious cycle” between the gut and the kidney.
1. Heal the Barrier (Assimilation & Defense)
To stop the “drip of poison,” we must seal the gut and shift the microbiome.
- The Solution: High-Fiber “Prebiotic” Therapy. Specific fibers (like acacia or partially hydrolyzed guar gum) feed the “good” bacteria that produce Butyrate. I also recommend the use of a continuous glucose monitor (CGM) to detect glucose spikes that might also carry a “renal tax”
- The Mechanism: Butyrate acts as a “cellular glue” for the tight junctions in the gut, reducing LPS translocation and shutting down the TLR4/NF-κB inflammatory alarm.
- The Result: Lower systemic inflammation and a reduced workload for the immune system.
2. Absorb the Toxins (Detoxification & Elimination)
When the kidney “exit” is slow, we can use the gut as a secondary filter.
- The Solution: Oral “Uremic Binders.” Medical-grade activated charcoal or specific carbon-based binders can “trap” toxins like Indoxyl Sulfate while they are still in the gut.
- The Mechanism: By binding these toxins before they are ever “assimilated,” we prevent them from reaching the liver. This relieves the “silencing” of CYP450 enzymes.
- The Result: Improved drug metabolism, reduced skin itching, and clearer cognitive function.
3. Support the Power Plants (Energy & Transport)
We must protect the mitochondria from the oxidative “exhaust” of uremic toxins.
- The Solution: Mitochondrial Resuscitation (CoQ10 & L-Carnitine). These nutrients are often depleted in CKD.
- The Mechanism: CoQ10 helps bypass the blocks in the Electron Transport Chain (Complex I/III), while L-Carnitine helps the mitochondria “burn” fat for fuel more efficiently.
- The Result: Improved ATP production, which helps combat sarcopenia (muscle wasting) and the profound fatigue of Stage 4.
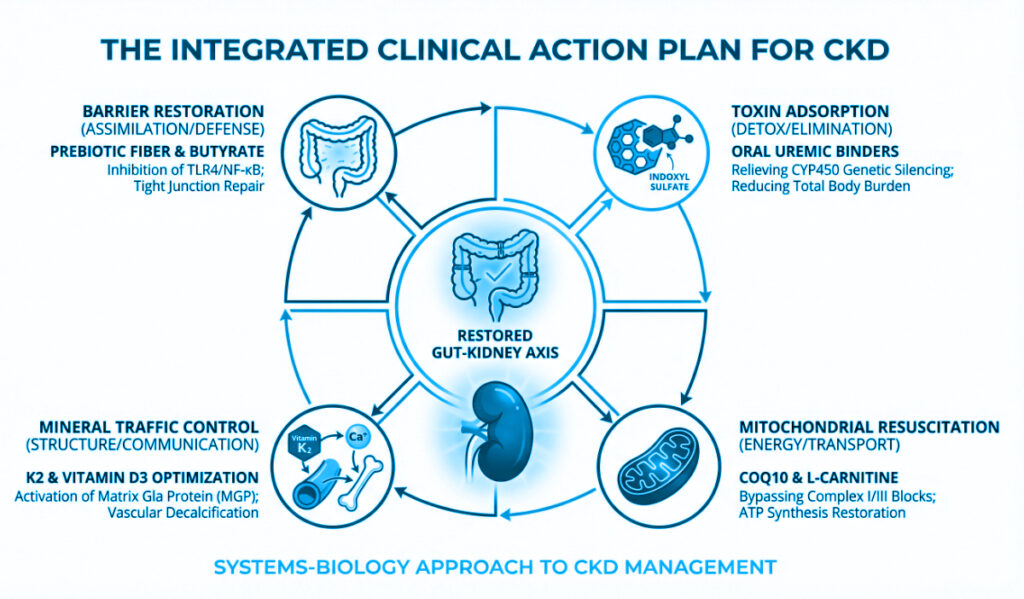
4. Restore the Peace (Communication & Structure)
We need to stop the “Mineral Migration” that destroys bones and stiffens arteries.
- The Solution: Vitamin K2 and Vitamin D Optimization. * The Mechanism: While Vitamin D helps with calcium absorption, Vitamin K2 (specifically MK-7) acts as the “Traffic Cop.” It activates a protein called Matrix Gla Protein (MGP), which physically inhibits calcium from settling in the blood vessels.
- The Result: Calcium stays in the Structure node (bones) and stays out of the Transport node (arteries), protecting the heart.
Conclusion – The Matrix as a Map for Recovery
By looking at CKD through these seven nodes, we see that the patient isn’t just a “failing kidney.” They are a complex system facing a Total Body Burden and an Integration: how Assimilation (Leaky Gut) fuels Defense (Inflammation), which damages Transport (eNOS/Vessels), poisons Energy (Mitochondria), silences Detoxification (CYP450), confuses Communication (Hormones), and finally dismantles Structure (Bones/Arteries).
Living with CKD can feel like a series of inevitable declines, but through the lens of the IFM Matrix, we see a different story—one of opportunity and intervention. By addressing the “toxic dialogue” between the gut and the kidneys, we move beyond simply monitoring lab values like GFR and Creatinine. We begin to actively restore the Energy in the cells, the Structure of the bones, and the Communication of hormones. This systems-biology approach is not a “quick fix,” but a strategic partnership with me to lower total body burden and reclaim quality of life.
My goal is to help you navigate this matrix, turning clinical complexity into a clear, actionable path toward systemic resilience. If you or someone you know suffers from CKD do not hesitate to schedule a complimentary discovery call.
